How Virtual Contrast Supervision Fills Physician Coverage Gaps Without a Full-Time Hire


Every imaging center administrator running contrast studies has done this math, or tried to. You need a qualified physician immediately available during contrast administration. Your current arrangement — a part-time physician, a traveling radiologist, a shared arrangement with a nearby practice — has gaps. You have weighed hiring a full-time radiologist. You have looked at locum tenens rates. You have considered restricting contrast studies to the days when coverage is confirmed. None of these options fully works, and all of them cost more than you would like.
The Problem You Are Actually Solving
Before comparing costs, it is worth being precise about what problem is on the table. The CMS direct supervision requirement for contrast-enhanced imaging — CT with IV contrast, contrast MRI, and similar studies — specifies that a qualified physician must be immediately available during contrast administration. Under the permanent rule effective January 1, 2026, “immediately available” includes real-time virtual presence via audio-visual connection. But the requirement does not go away.
For urban or suburban imaging facilities with multiple physicians on staff, this is a non-issue. For facilities operating with thin or unpredictable coverage — which describes a large share of community, rural, and independent imaging centers — meeting this requirement is a daily operational variable. When it cannot be met, contrast studies cannot proceed.
The contrast supervision gap is not a general staffing question. It is a specific compliance question with a specific operational consequence: the scan either happens with compliant supervision, or it does not happen. There is no partial solution. That specificity matters for evaluating the options, because a full-time radiologist hire is not primarily a contrast supervision strategy. It is a comprehensive clinical and operational investment that incidentally closes the supervision gap. Virtual contrast supervision is the targeted instrument. Understanding the difference shapes how you evaluate the cost.
What a Full-Time Radiologist Actually Costs
The sticker price for a radiologist is already among the highest in medicine, and it is the starting point for a cost structure that runs considerably higher.
Base compensation
Based on 2025 and 2026 compensation data from Medscape, Doximity, and SalaryDr, the average total compensation for a diagnostic radiologist in the United States currently falls between $520,000 and $585,000 annually, depending on the source methodology. Outpatient imaging centers specifically tend to sit toward the higher end of that range — $500,000 to $600,000 — partly because they compete with larger hospital systems that can offer more comprehensive benefit structures. These figures are for base compensation plus bonuses; they do not include the cost of employing the physician.
The loaded cost beyond salary
For a facility employing a full-time radiologist directly, total cost of employment is materially higher than the base figure:
- Benefits package: Health insurance, dental, vision, and retirement contributions add an estimated $20,000 to $40,000 annually for a physician-level employee, depending on the plan and match structure.
- Malpractice insurance: Radiology malpractice premiums vary by state and practice setting but typically run $10,000 to $30,000 annually for a diagnostic radiologist, with tail coverage adding additional cost if the physician leaves.
- CME and licensing: Continuing medical education allowances typically run $3,000 to $5,000 annually. Multi-state licensing and credentialing fees add further overhead, particularly for facilities in states with complex licensing requirements.
- Recruitment and onboarding: Per the Association for Advancing Physician and Provider Recruitment, it takes an average of 130 days to fill a full-time radiology position. Search firm fees, relocation packages, signing bonuses, and the administrative cost of credentialing add a one-time cost that is frequently in the range of $30,000 to $100,000 for a specialty physician hire.
- Ongoing HR overhead: Annual reviews, HR compliance, scheduling management, and the cost of coverage during the employee’s own vacation and continuing education time create an overhead that is not reflected in the base salary figure.
A conservative total-cost-of-employment estimate for a full-time diagnostic radiologist at a community imaging center lands at $580,000 to $700,000 or more per year. In a market where 50% of radiology job openings went unfilled in 2023 and where the average position takes more than four months to fill, that cost is not always accessible even when the budget exists for it.
What Locum Tenens Coverage Actually Costs
Locum tenens is the most common gap-filling strategy for imaging facilities that cannot recruit or afford a full-time radiologist. It has real utility — but it is not cheap, and it has limitations that are frequently underestimated.
Locum rates for contrast supervision coverage
Locum tenens diagnostic radiologists currently earn in the range of $250 to $330 per hour in most markets, with rates running higher in rural or underserved areas where demand exceeds supply — facilities in high-need areas sometimes see premiums of 20% to 40% above standard rates for immediate deployment. At $280 per hour with a modest eight-hour shift, a single day of locum coverage runs $2,240 before the agency margin and any travel or housing costs the facility is responsible for absorbing.
Annualized across a five-day-per-week schedule, locum tenens coverage at $280 per hour for eight hours daily totals roughly $582,000 in physician time alone. For most facilities, the gap they are trying to fill is not a full week — it is specific days, specific hours, and unplanned absences. But the per-day cost does not scale downward proportionally; unplanned, short-notice locum coverage commands premium rates.
The hidden costs of locum arrangements
Beyond the hourly rate, locum tenens arrangements carry structural costs that are easy to underestimate when evaluating a simple day-rate figure:
- Agency fees: Staffing agencies typically mark up physician placement costs by 20% to 40% above the rate paid to the physician. The rate you pay is not the rate the physician receives.
- Credentialing lead time: Credentialing a locum physician at a new facility typically takes 60 to 90 days. For planned coverage gaps, this is manageable. For unplanned absences, it is not. A locum who was not pre-credentialed cannot be deployed on short notice.
- Continuity and familiarity costs: A rotating locum does not know your workflows, your technologists, or your patient population. Every new locum requires an orientation period that reduces efficiency and introduces quality variation.
- Unreliability on short notice: Locum coverage is scheduled in advance. When your covering physician calls out unexpectedly — which is precisely the failure mode that creates the most operational damage — the locum pool is not a same-day solution.
The operational gap: Locum tenens covers planned gaps. Virtual contrast supervision covers all gaps, including unplanned ones, across all operating hours, without credentialing lead time or per-day rate variability.
What Virtual Contrast Supervision Provides Instead
Virtual contrast supervision through ContrastConnect is not a physician staffing product. It does not place a physician at your facility. What it provides is a contracted service under which a qualified, board-certified physician supervises contrast administration in real time via a live audio-visual connection that satisfies the CMS direct supervision standard — for every contrast study, across all your operating hours, with 100% coverage fulfillment on requested hours.
The comparison to a full-time hire or a locum arrangement needs to be made precisely: virtual supervision addresses one specific compliance function — direct supervision during contrast administration — and it addresses it comprehensively and at predictable cost.
What it replaces, specifically
For an imaging center that has been managing contrast supervision through a part-time or locum physician:
- The physician’s presence is no longer needed on-site for contrast administration. Your technologist performs the procedure; the virtual supervising physician is immediately available via live connection throughout.
- Coverage is no longer dependent on whether a specific individual is available on a specific day. An unplanned absence does not cascade into cancelled contrast scans.
- Evening and weekend contrast imaging becomes operationally feasible across all hours, without a physician scheduled on-site for those shifts.
- Documentation of supervision is generated automatically through the platform, supporting audit readiness without additional administrative burden.
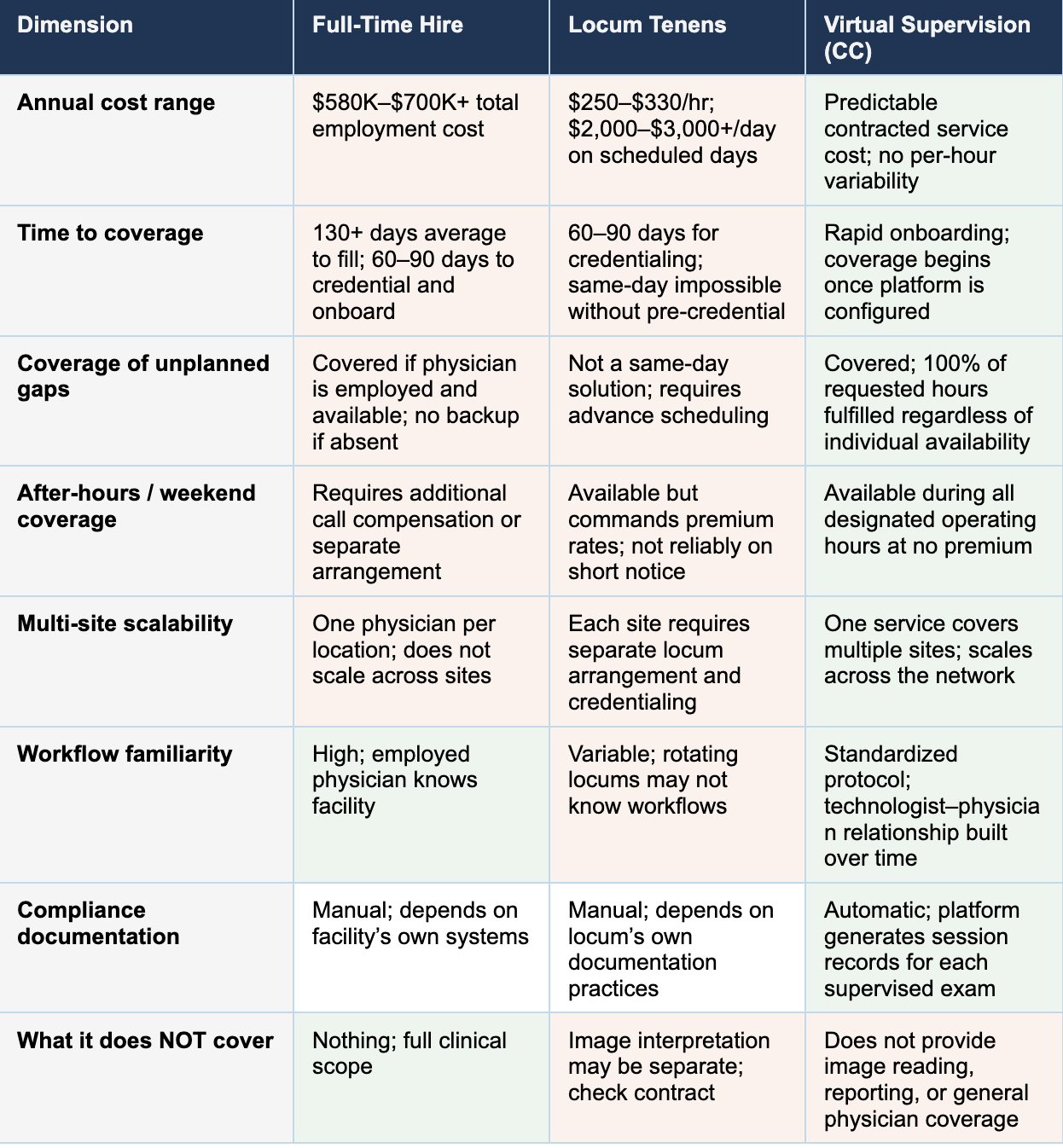
Side-by-Side: Full-Time Hire vs. Locum vs. Virtual Supervision
The table below compares the three primary approaches along the dimensions that matter most to an operations director evaluating contrast supervision coverage.
The Coverage Gap Has a Targeted Solution
If you are the operations director of a community imaging center managing contrast supervision through arrangements that leave you one unexpected absence away from a cancelled schedule, the options in front of you are not equally good. A full-time hire is expensive, slow to recruit, and more than you need for this specific function. A locum covers scheduled days and nothing else. Restricting contrast imaging to days when coverage is confirmed shrinks your service capacity to match your staffing constraints.
Virtual contrast supervision is the instrument designed for exactly this problem. It fulfills 100% of requested coverage hours. It operates across your full schedule, including evenings and weekends. It generates automatic compliance documentation. It scales across multiple sites. And it eliminates the cancellation cascade that follows every unexpected physician absence.
ContrastConnect’s team works with imaging centers of every size and configuration to structure coverage that fits the facility’s workflow and operating hours. If your contrast supervision model has gaps, we would like to show you what closing them looks like.
Trusted Nationwide

















.avif)




1,000,000
Contrast exams supervised annually
75,000+
Hours of supervision monthly
3,900+
Technologists certified
100s
Of imaging partners nationwide
130+
Contrast reactions treated monthly
100%
Requested hours covered
Connect with us.

